Staging is a measure of the degree to which the cancer has spread. Cancer spreads microscopically and grows into tumors at new locations. The number, location and size of these new tumors can give a sense of the degee to which the cancer is contained to a limited location. Clearly, even when there is just one small tumor in the abdomen (Stage II), there could still be microscopic disease elsewhere. But the likelihood is less than when the tumor is large or there are several tumors or there are tumors outside the abdomen. Thus the staging of the cancer can help the doctor choose an appropriate treatment. Localized treatments like radiation therapy and surgery can be used in the early stages, which systemic treatments like chemotherapy can be used in the later stages.
Staging is usually accomplished through a CT scan. A CT scan, also known as a CAT scan, is a series of X-ray images representing slices of the body. In the case of testicular cancer, usually the CT scan will be limited to the pelvis, abdomen, and chest. Before the CT scan, you will have to drink two quarts of milky white barium sulfate solution which will make you feel like you need to vomit. Typically they will take one series of images without contrast die and one with contrast die. The contrast die is injected into your vein through an IV. When the contrast die is in your system, you will be able to feel the X-rays operating because you will feel very hot. Do not be surprised if you need to go to the bathroom urgently about an hour after the CT scan.
The following images show examples of CT scans. The red arrows indicate the metastasized tumors. Click on any image for an enlargment.
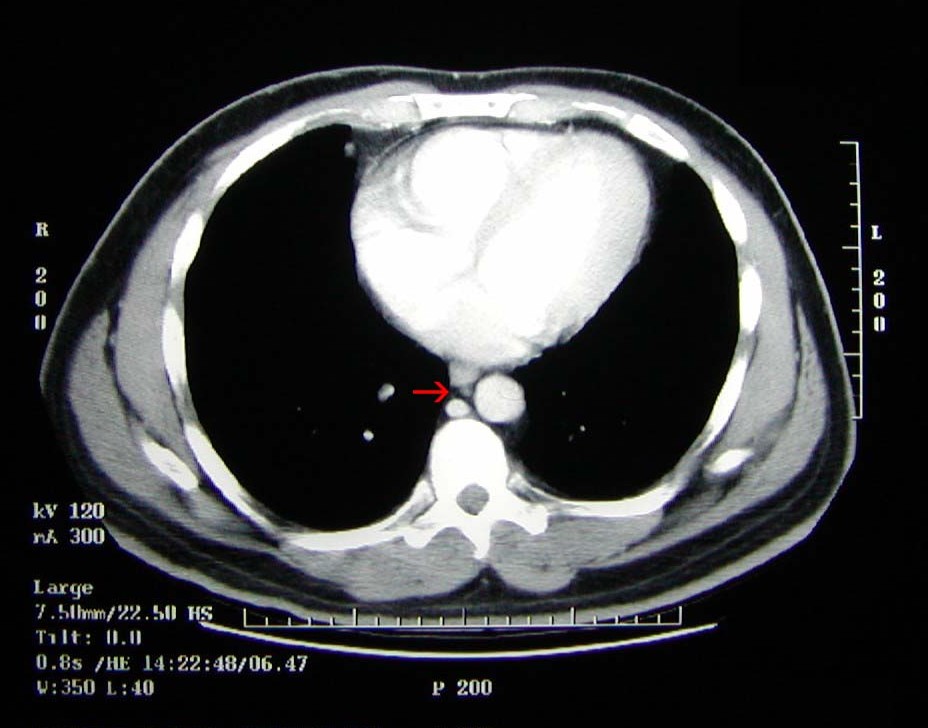 Chest CT Scan. This image shows a 5 mm tumor in the right cardiophrenic lymph node adjacent to the heart. The existence of a tumor in the chest indicates stage III testicular cancer. |
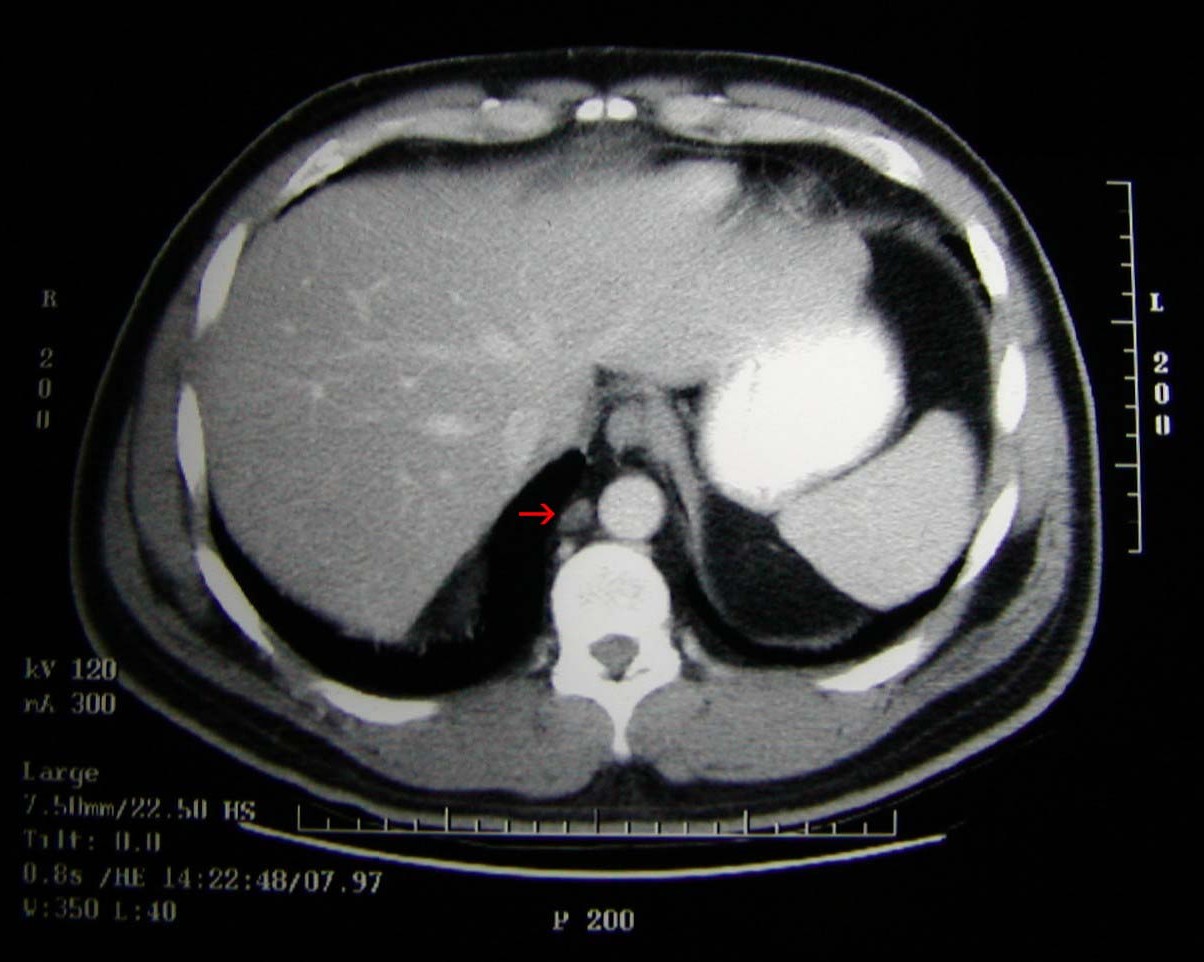 Chest CT Scan. This image shows a 1 cm tumor in the right retrocrural lymph node. The existence of a tumor in the chest indicates stage III testicular cancer. |
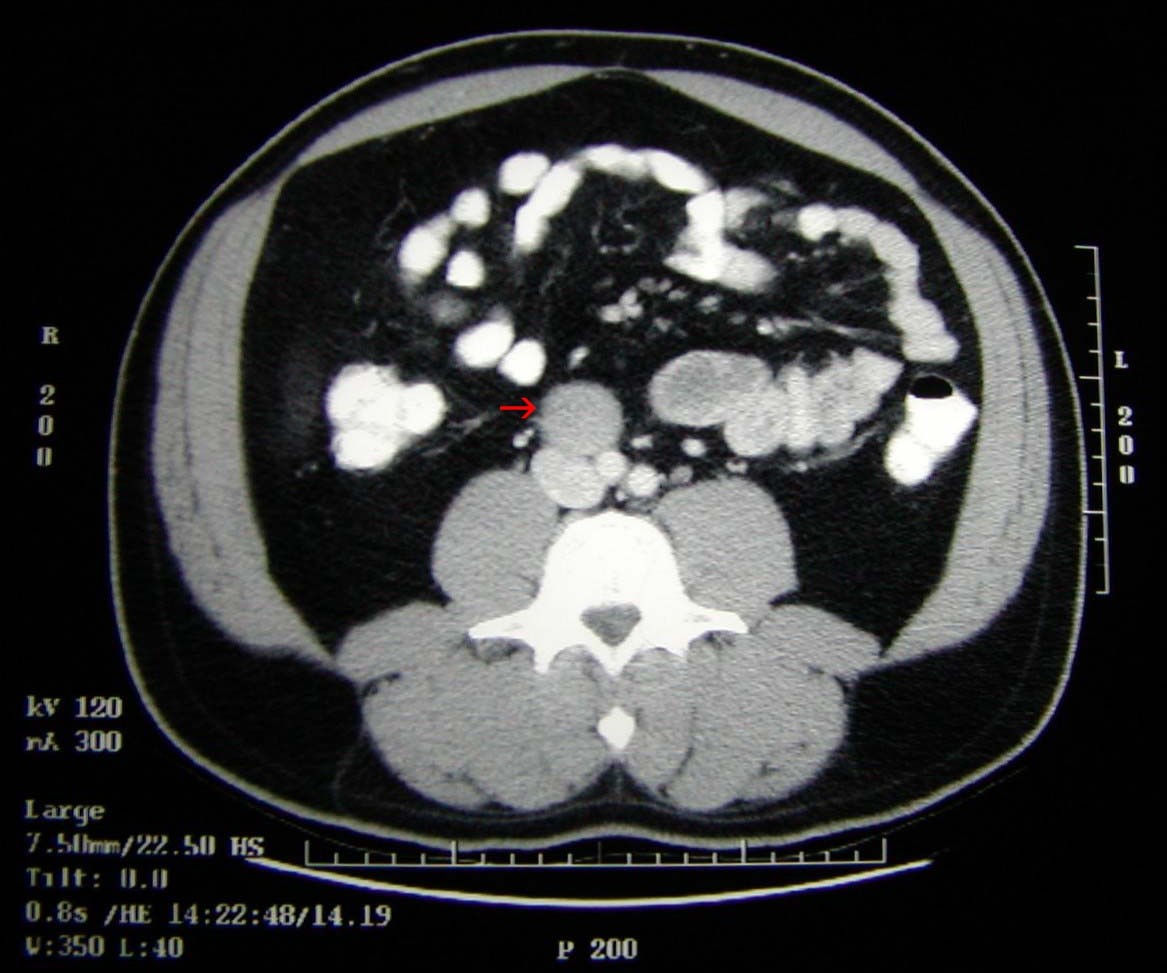 Abdominal CT Scan. This image shows a 3 cm nodal mass at the level of the aortic bifurcation (where the aorta splits to go into the legs). |
A chest X-ray is often used to determine whether the cancer has spread to the lungs.
Sometimes serum tumor markers are also used to determine the staging and monitor the response to treatment. Serum tumor markers are substances in the blood or urine that are present in higher than normal amounts in people with certain types of testicular cancer, such as non-seminoma cancers. Serum tumor markers include human chorionic gonadotrophin (beta-HCG), alpha-fetoprotein (AFP), and lactic dehydrogenase (LDH). 85% of non-seminomas show elevated levels of beta-HCG or AFP.
The major stages are as follows:
- Stage I (Local). The cancer is limited to the testicles and has not spread to the lymph nodes or a more distant organ. Approximately 72% of testicular cancers are in Stage I.
- Stage II (Regional). The cancer has spread to the lymph nodes in the abdomen, but not to a more distant organ. Approximately 19% of testicular cancers are in Stage II.
- Stage III (Distant). The cancer has spread to the lymph nodes and one or more distant organs (above the diaphragm), such as the liver, lungs and brain. Approximately 9% of testicular cancers are in Stage III.
Impact of Staging on Treatment
The results of the pathology report and the staging CT scan will determine treatment options. Stage I patients often have the option of surveillance (no active treatment, but monitor for signs of relapse), radiation therapy (seminoma) or chemotherapy (non-seminoma). Stage II patients are usually given the option of radiation therapy (seminoma) or chemotherapy (non-seminoma), but may also be given the option of a RPLND (surgical removal of the lymph nodes). The only option for stage III patients is chemotherapy.
Prognosis
In the following table, the LDH scores represent the ratio of the LDH value to the upper limit of the laboratory's normal range.
| Risk Status | Nonseminoma | Stages | Seminoma | Stages |
| Good Prognosis | No nonlung spread Good markers AFP < 1,000 HCG < 5,000 LDH < 1.5 |
IS (S1) IIA (S1) IIB (S1) IIC (S1) IIIA |
No nonlung spread AFP normal HCG and LDH can be any level |
IIC IIIA IIIB IIIC |
| Intermediate Prognosis | No nonlung spread Intermediate markers AFP 1000 -10,000 HCG 5000 - 50,000 LDH 1.5 - 10 |
IS (S2) IIC (S2) IIIB |
Nonlung spread AFP normal HCG and LDH can be any level |
IIIC with Non lung spread |
| Poor Prognosis | Nonlung spread High markers AFP >10,000 HCG > 50,000 LDH > 10 |
IS (S3) IIC (S3) All IIIC |
None |
Current cure rates for testicular cancer are as follows:
| Stage | Seminoma | Non-Seminoma | Overall |
| Stage I | 99% | 98% | 98% |
| Stage II | 95% | 95% | 95% |
| Stage III | 90% | 76% | 78% |
| All Stages | 96% |
Causes | Checklist | Costs | Cancer Jokes | Cancer Scholarships | Sites